Muscles Of The Upper Limb Labeled
Muz Play
Mar 21, 2025 · 7 min read
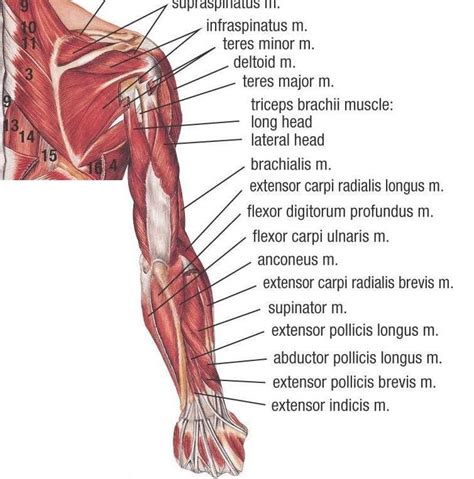
Table of Contents
Muscles of the Upper Limb: A Comprehensive Guide with Labeled Diagrams
The upper limb, encompassing the arm, forearm, and hand, boasts a complex network of muscles crucial for a wide range of movements. From the delicate dexterity required for writing to the powerful strength needed for lifting, understanding the individual muscles and their functions is key to appreciating the intricate biomechanics of this remarkable part of the human body. This comprehensive guide will delve into the muscles of the upper limb, providing detailed descriptions, functions, and labeled diagrams for better understanding. We'll explore each region systematically, focusing on their anatomical location, actions, innervation, and clinical relevance.
I. Muscles of the Shoulder Region
The shoulder region, where the upper limb articulates with the trunk, houses a group of muscles responsible for a wide array of movements including abduction, adduction, flexion, extension, medial and lateral rotation, and circumduction. These muscles can be broadly categorized into those originating from the axial skeleton (stabilizing the shoulder girdle) and those originating from the scapula (directly involved in shoulder joint movement).
A. Muscles Originating from the Axial Skeleton:
-
Pectoralis Major: This large, fan-shaped muscle originates from the clavicle, sternum, and costal cartilages and inserts onto the greater tubercle of the humerus. Actions: Flexion, adduction, and medial rotation of the humerus. It also assists in forced inspiration. Innervation: Medial and lateral pectoral nerves. Clinical Relevance: Pectoralis major tears are common in athletes, particularly in contact sports.
-
Pectoralis Minor: A smaller muscle located deep to the pectoralis major, it originates from ribs 3-5 and inserts onto the coracoid process of the scapula. Actions: Protraction, depression, and downward rotation of the scapula. Innervation: Medial pectoral nerve. Clinical Relevance: Pectoralis minor syndrome can cause pain in the chest and shoulder.
-
Subclavius: A small muscle located deep to the clavicle, it originates from the first rib and inserts onto the clavicle. Actions: Depresses and protracts the clavicle. Innervation: Nerve to subclavius. Clinical Relevance: Rarely involved in clinical presentations.
-
Serratus Anterior: This muscle originates from the upper eight ribs and inserts onto the medial border of the scapula. Actions: Protraction, upward rotation, and abduction of the scapula. Innervation: Long thoracic nerve. Clinical Relevance: Damage to the long thoracic nerve (e.g., during surgery) can result in "winged scapula," where the medial border of the scapula protrudes.
B. Muscles Originating from the Scapula:
-
Deltoid: A large, powerful muscle covering the shoulder joint, it originates from the clavicle, acromion, and spine of the scapula and inserts onto the deltoid tuberosity of the humerus. Actions: Anterior fibers: flexion and medial rotation; middle fibers: abduction; posterior fibers: extension and lateral rotation of the humerus. Innervation: Axillary nerve. Clinical Relevance: Deltoid muscle tears are common injuries, particularly in athletes.
-
Supraspinatus: Located above the spine of the scapula, it originates from the supraspinous fossa and inserts onto the greater tubercle of the humerus. Actions: Abduction of the humerus (initiates abduction). Innervation: Suprascapular nerve. Clinical Relevance: Supraspinatus tendinitis and rotator cuff tears are frequent sources of shoulder pain.
-
Infraspinatus: Located below the spine of the scapula, it originates from the infraspinous fossa and inserts onto the greater tubercle of the humerus. Actions: Lateral rotation of the humerus. Innervation: Suprascapular nerve. Clinical Relevance: Infraspinatus tendinitis and rotator cuff tears.
-
Teres Minor: A small muscle located inferior to the infraspinatus, it originates from the lateral border of the scapula and inserts onto the greater tubercle of the humerus. Actions: Lateral rotation of the humerus. Innervation: Axillary nerve. Clinical Relevance: Often involved in rotator cuff tears.
-
Subscapularis: Located on the anterior surface of the scapula, it originates from the subscapular fossa and inserts onto the lesser tubercle of the humerus. Actions: Medial rotation of the humerus. Innervation: Upper and lower subscapular nerves. Clinical Relevance: Subscapularis tendinitis and rotator cuff tears. (Note: Supraspinatus, infraspinatus, teres minor, and subscapularis together comprise the rotator cuff muscles).
II. Muscles of the Arm
The arm, extending from the shoulder to the elbow, primarily contains muscles acting on the elbow joint. These muscles can be grouped into anterior (flexors) and posterior (extensors) compartments.
A. Anterior Compartment (Flexors):
-
Biceps Brachii: A two-headed muscle originating from the coracoid process (short head) and supraglenoid tubercle of the scapula (long head), it inserts onto the radial tuberosity. Actions: Flexion of the elbow, supination of the forearm, and weak flexion of the shoulder. Innervation: Musculocutaneous nerve. Clinical Relevance: Biceps tendon rupture is a common injury, particularly in older individuals.
-
Brachialis: Located deep to the biceps brachii, it originates from the anterior surface of the humerus and inserts onto the ulnar tuberosity. Actions: Flexion of the elbow. Innervation: Musculocutaneous nerve. Clinical Relevance: Less frequently injured compared to other elbow flexors.
-
Coracobrachialis: A small muscle originating from the coracoid process of the scapula and inserting onto the medial surface of the humerus. Actions: Flexion and adduction of the humerus. Innervation: Musculocutaneous nerve. Clinical Relevance: Relatively infrequent clinical significance.
B. Posterior Compartment (Extensors):
- Triceps Brachii: A three-headed muscle originating from the infraglenoid tubercle of the scapula (long head), posterior surface of the humerus (lateral and medial heads), it inserts onto the olecranon process of the ulna. Actions: Extension of the elbow, and extension and adduction of the shoulder (long head). Innervation: Radial nerve. Clinical Relevance: Triceps tendon rupture is less common than biceps rupture but can occur, particularly with forceful contractions.
III. Muscles of the Forearm
The forearm muscles are complex, grouped into anterior (flexors), posterior (extensors), and lateral compartments based on their location and function. Many of these muscles act on the wrist, hand, and fingers.
A. Anterior Compartment (Flexors):
This compartment contains several layers of muscles, with superficial muscles primarily flexing the wrist and deep muscles predominantly flexing the fingers. Examples include:
- Flexor carpi radialis: Flexion and radial deviation of the wrist.
- Palmaris longus: Weak flexion of the wrist (often absent).
- Flexor carpi ulnaris: Flexion and ulnar deviation of the wrist.
- Flexor digitorum superficialis: Flexion of the proximal interphalangeal joints of the fingers.
- Flexor digitorum profundus: Flexion of the distal interphalangeal joints of the fingers.
- Flexor pollicis longus: Flexion of the thumb.
Innervation: Primarily median nerve (except flexor carpi ulnaris and flexor digitorum profundus medial half, innervated by ulnar nerve).
B. Posterior Compartment (Extensors):
Similar to the anterior compartment, this contains multiple layers with superficial muscles extending the wrist and deep muscles extending the fingers. Key muscles include:
- Extensor carpi radialis longus and brevis: Extension and radial deviation of the wrist.
- Extensor carpi ulnaris: Extension and ulnar deviation of the wrist.
- Extensor digitorum: Extension of the metacarpophalangeal and interphalangeal joints of the fingers.
- Extensor indicis: Extension of the index finger.
- Extensor digiti minimi: Extension of the little finger.
- Extensor pollicis longus and brevis: Extension of the thumb.
- Abductor pollicis longus: Abduction of the thumb.
Innervation: Primarily radial nerve.
C. Lateral Compartment:
This compartment contains muscles involved primarily in thumb movements:
- Brachioradialis: Flexion of the elbow.
- Supinator: Supination of the forearm.
Innervation: Radial nerve.
IV. Muscles of the Hand
The intrinsic muscles of the hand are small and complex, responsible for fine motor control and dexterity. They are located within the hand and act on the fingers and thumb. They are organized into thenar (thumb), hypothenar (little finger), and midpalmar (central) compartments. Detailed descriptions of each intrinsic muscle are beyond the scope of this overview. However, understanding their general functions is crucial:
- Thenar muscles: Responsible for thumb opposition, abduction, adduction, and flexion.
- Hypothenar muscles: Responsible for little finger abduction, flexion, and opposition.
- Midpalmar muscles: Lumbricals and interossei muscles that flex the metacarpophalangeal joints and extend the interphalangeal joints of the fingers, also involved in finger adduction and abduction.
Innervation: Median, ulnar, and radial nerves.
V. Clinical Relevance and Conclusion
Understanding the muscles of the upper limb is vital for clinicians in diagnosing and managing a wide range of conditions, including fractures, sprains, strains, nerve injuries, and tendinitis. Many injuries are sports related, focusing on the rotator cuff, biceps, and triceps, while others are due to repetitive strain or overuse. Accurate diagnosis relies on a thorough knowledge of muscle anatomy, function, and innervation. This guide provides a foundational overview, but further exploration through detailed anatomical texts and clinical resources is recommended for a comprehensive understanding. The complex interplay of these muscles allows for the incredible range of motion and dexterity characterizing the human upper limb, a testament to the remarkable efficiency of human musculature. Remember always to consult with healthcare professionals for any concerns regarding pain or injuries in the upper limb.
Latest Posts
Latest Posts
-
How Does Thermal Energy Affect The 3 States Of Matter
Mar 21, 2025
-
Is Solubility A Chemical Or Physical Property
Mar 21, 2025
-
What Are Vertical Columns On The Periodic Table Called
Mar 21, 2025
-
What Is The Stage On A Microscope
Mar 21, 2025
-
Dimensional Analysis Problems With Answers Pdf
Mar 21, 2025
Related Post
Thank you for visiting our website which covers about Muscles Of The Upper Limb Labeled . We hope the information provided has been useful to you. Feel free to contact us if you have any questions or need further assistance. See you next time and don't miss to bookmark.
